Pre-Trip Driver Medical Checkups
Digital pre-trip medical screening system with USB-synchronized breathalyzer integration.
Quick read
Ukrainian commercial drivers require a pre-trip medical check before each shift: pulse, blood pressure, temperature, and breathalyzer reading, all logged in a paper journal. As one of the physicians performing these checks, I built a digital system that replaces the journal — the medic enters readings on a web app, plugs the Drager iBlow 10 breathalyzer into USB at end-of-shift, and a desktop agent reconciles software-entered records with the device's onboard memory using time-windowed matching to confirm legitimacy. Production-grade: AES-256 encryption on medical fields, JWT auth, signed PDFs with JKS-based electronic signature, row-level multi-tenancy. Functional today; the regulatory path to replacing the paper journal is open but uncertain.
Context
Ukrainian law requires commercial drivers to undergo a pre-trip medical exam before each shift. The medic on duty measures pulse, blood pressure, body temperature, and uses a breathalyzer (Drager-brand or equivalent) to confirm sobriety. Each reading is logged in a paper journal with the driver's name, time, and the medic's signature.
The paper journal is the legal artifact. It's auditable by transport regulators, retained for years, and serves as proof that the check was performed correctly.
Two problems with the paper status quo:
- Reconciliation is manual. The breathalyzer device stores its own internal readings log. The paper journal records what the medic wrote down. There's no enforced link between the two — a journal can be filled in without an actual breathalyzer test, or vice versa.
- It's slow. Logging by hand across pulse, BP, temperature, BAC for each driver, multiplied across a shift, eats into the medic's time and increases transcription errors.
I perform these checks regularly as part of my work. I built the digital system to solve both problems for my own use, with a path to broader deployment if I can get it certified as a legal replacement for the paper journal.
Solution
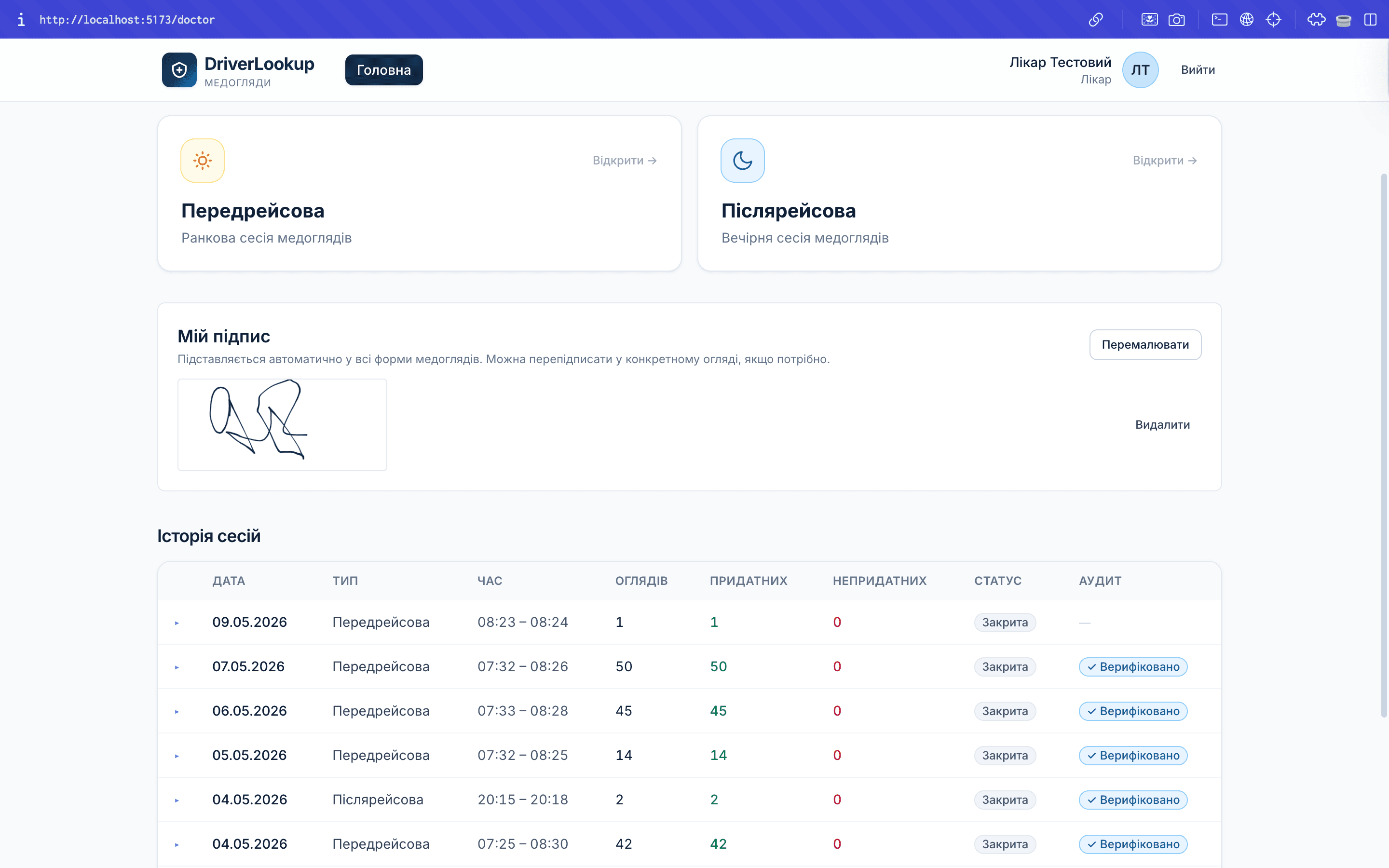
A computer-based system where the medic logs each driver's pre-trip check digitally (pulse, BP, temperature, BAC reading, time, driver identity). At the end of a shift, the Drager breathalyzer plugs into USB and the system reads the device's internal log directly.
The system then reconciles: for every BAC reading the medic entered in software, the corresponding reading should exist in the device's onboard memory at approximately the same time. A check is "verified" only when both records match. Mismatches are flagged.
This produces a legitimacy claim that paper can't: the digital log isn't just what the medic claims happened — it's what the medic claimed and what the device recorded, cross-referenced.
The function works end-to-end today. What's open is regulatory: legally replacing the paper journal requires authorization from the institutions that mandated the paper form (Ministry of Health and Ministry of Internal Affairs). I've been through the initial outreach with MoH and NSZU, which directed me to file a formal public inquiry with the authorizing ministries — a process with a 30-day nominal response window but unreliable in practice.
Impact
The system is in functional production at my own workplace but cannot yet legally replace the paper journal — so today it runs alongside paper rather than replacing it. The deployment story will be told properly once regulatory approval is in place.
What the system already proves:
- The cross-referencing approach works technically. USB sync against the Drager iBlow 10's internal memory produces a clean time-windowed reconciliation log per shift.
- A reverse-engineered USB protocol is a sustainable foundation. The vendor publishes Windows-only software; macOS support was traced manually with a USB sniffer. The protocol now lives in ~500 LOC of TypeScript inside an Electron menu-bar agent.
- The compliance gap is regulatory, not technical. The paper journal exists because the law says so, not because the workflow needs it. The system already implements what a regulatory-ready electronic equivalent would need: AES-256-GCM encryption of medical fields, JWT auth with brute-force lockout, electronic signatures on PDF acts via JKS-based pyHanko signing, full audit log with signing IP and user-agent, row-level multi-tenancy via
organization_id, and per-shift device memory dumps stored for verification.
Working code that's not legally usable is, for compliance products, indistinguishable from working code that doesn't exist.
What I learned
- Reverse-engineering a vendor USB protocol is a tractable solo project if you commit to the boring part. Drager publishes the iBlow 10 with macOS no-go status — software exists only for Windows. To map the protocol I borrowed a Windows laptop, installed a USB sniffer, and ran traffic between the official client and the device for several hours while triggering every operation I could. With enough capture data, the protocol shape emerged. The lesson isn't about USB — it's about timeboxing: most "we'd need vendor access" problems are actually "we'd need a weekend with a sniffer" problems.
- Time-windowing was the right abstraction for cross-device reconciliation. I started by trying to match by content (BAC value) and quickly realized that two consecutive drivers with similar readings would alias. Matching by timestamp alone has the same issue if device clock drifts. The breakthrough was reframing: don't match individual records, match windows-and-records. Each exam is a window owned by the medic's UI; each device record is a point in time; one window owns one point. Mismatches are anomalies. This generalized into a clean audit log: every legal record has a verifiable provenance pair.
- Regulatory inertia is a real product risk and worth pricing in early. Working code that's not legally usable is, for compliance products, indistinguishable from working code that doesn't exist. To replace the paper journal, an electronic system needs sign-off from the institutions that authorized the paper form — Ministry of Health and Ministry of Internal Affairs. The official channel is a public inquiry; the official response window is ~30 days. In practice, my previous public inquiry to MoH went unanswered for months. I now treat regulatory feedback time as a hard input to the product roadmap, not a polite assumption. For future compliance-bound builds, I'd start the regulatory conversation before the code.
Next steps
The active decision is not about the deployment track — Caddy + HTTPS, containerized backend, backups are scoped and could ship — but about product surface. With regulatory feedback slow and uncertain, I'm looking for a surface where the same architecture (encrypted medical fields, signed PDFs, USB device sync, multi-tenancy) maps to a use case that doesn't require ministerial approval. A concrete candidate is extending the agent to handle a Bluetooth pulse oximeter — same reconciliation model, broader applicability beyond the transport-medic context. That's a direction, not a commitment yet.
The parallel path is still open: production deployment as a legally-usable replacement for the paper journal once MoH and MIA respond to the public inquiry defining requirements for an electronic equivalent. Until they do, parallel running has limited value over the paper alone, so the working assumption is that the second product surface is the near-term move.
Read next